
Article, FEATURED STORIES, news, WORLD
WHO Updates COVID-19 Transmission Information After New Evidence Arises, Airborne Transmission Possible
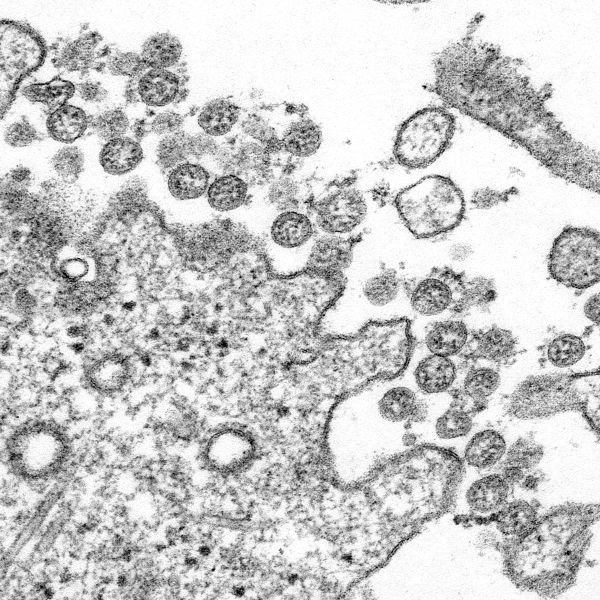
Transmission electron microscopic image of an isolate from the first U.S. case of COVID-19, formerly known as 2019-nCoV. The spherical extracellular viral particles contain cross-sections through the viral genome, seen as black dots
After recent research found within the scientific community showing airborne transmission is likely, an international group of epidemiologists and scientists approached the World Health Organization (WHO) with a request to review their COVID-19 (Coronavirus, 2019) transmission guidelines.
The request came as WHO discontinued the treatment arms for hydroxychloroquine and lopinavir/ritonavir testing. “WHO today accepted the recommendation from the Solidarity Trial’s International Steering Committee to discontinue the trial’s hydroxychloroquine and lopinavir/ritonavir arms. The Solidarity Trial was established by WHO to find an effective COVID-19 treatment for hospitalized patients,” read a recent press release from the organization.
The press release would continue:
These interim trial results show that hydroxychloroquine and lopinavir/ritonavir produce little or no reduction in the mortality of hospitalized COVID-19 patients when compared to standard of care. Solidarity trial investigators will interrupt the trials with immediate effect.
For each of the drugs, the interim results do not provide solid evidence of increased mortality. There were, however, some associated safety signals in the clinical laboratory findings of the add-on Discovery trial, a participant in the Solidarity trial. These will also be reported in the peer-reviewed publication.
Regarding new transmission discovery, WHO updated its Transmission of SARS-CoV-2 [COVID-19]: implications for infection prevention precautions scientific brief.
Concerning ‘modes of transmission’ the brief details ‘Contact and droplet transmission,’ ‘Airborne transmission,’ ‘Fomite transmission,’ and ‘Other modes of transmission’ that aren’t as frequent.
Regarding ‘Contact and droplet transmission’:
Transmission of SARS-CoV-2 can occur through direct, indirect, or close contact with infected people through infected secretions such as saliva and respiratory secretions or their respiratory droplets, which are expelled when an infected person coughs, sneezes, talks or sings…Respiratory droplet transmission can occur when a person is in close contact (within 1 metre) with an infected person who has respiratory symptoms (e.g. coughing or sneezing) or who is talking or singing; in these circumstances, respiratory droplets that include virus can reach the mouth, nose or eyes of a susceptible person and can result in infection. Indirect contact transmission involving contact of a susceptible host with a contaminated object or surface (fomite transmission) may also be possible.
Regarding ‘Airborne transmission’:
Airborne transmission is defined as the spread of an infectious agent caused by the dissemination of droplet nuclei (aerosols) that remain infectious when suspended in air over long distances and time. Airborne transmission of SARS-CoV-2 [COVID-19] can occur during medical procedures that generate aerosols (“aerosol generating procedures”). WHO, together with the scientific community, has been actively discussing and evaluating whether SARS-CoV-2 may also spread through aerosols in the absence of aerosol generating procedures, particularly in indoor settings with poor ventilation.
The physics of exhaled air and flow physics have generated hypotheses about possible mechanisms of SARS-CoV-2 transmission through aerosols. These theories suggest that 1) a number of respiratory droplets generate microscopic aerosols (<5 µm) by evaporating, and 2) normal breathing and talking results in exhaled aerosols. Thus, a susceptible person could inhale aerosols, and could become infected if the aerosols contain the virus in sufficient quantity to cause infection within the recipient. However, the proportion of exhaled droplet nuclei or of respiratory droplets that evaporate to generate aerosols, and the infectious dose of viable SARS-CoV-2 required to cause infection in another person are not known, but it has been studied for other respiratory viruses.
Outside of medical facilities, some outbreak reports related to indoor crowded spaces have suggested the possibility of aerosol transmission, combined with droplet transmission, for example, during choir practice, in restaurants or in fitness classes. In these events, short-range aerosol transmission, particularly in specific indoor locations, such as crowded and inadequately ventilated spaces over a prolonged period of time with infected persons cannot be ruled out. However, the detailed investigations of these clusters suggest that droplet and fomite transmission could also explain human-to-human transmission within these clusters. Further, the close contact environments of these clusters may have facilitated transmission from a small number of cases to many other people (e.g., superspreading event), especially if hand hygiene was not performed and masks were not used when physical distancing was not maintained.
Regarding ‘Fomite transmission’:
Respiratory secretions or droplets expelled by infected individuals can contaminate surfaces and objects, creating fomites (contaminated surfaces). Viable SARS-CoV-2 virus and/or RNA detected by RT-PCR can be found on those surfaces for periods ranging from hours to days, depending on the ambient environment (including temperature and humidity) and the type of surface, in particular at high concentration in health care facilities where COVID-19 patients were being treated.
Despite consistent evidence as to SARS-CoV-2 contamination of surfaces and the survival of the virus on certain surfaces, there are no specific reports which have directly demonstrated fomite transmission. People who come into contact with potentially infectious surfaces often also have close contact with the infectious person, making the distinction between respiratory droplet and fomite transmission difficult to discern. However, fomite transmission is considered a likely mode of transmission for SARS-CoV-2, given consistent findings about environmental contamination in the vicinity of infected cases and the fact that other coronaviruses and respiratory viruses can transmit this way.
Regarding ‘Other modes of transmission’:
Some studies have reported the detection of SARS-CoV-2 RNA, in either plasma or serum, and the virus can replicate in blood cells. However, the role of bloodborne transmission remains uncertain; and low viral titers in plasma and serum suggest that the risk of transmission through this route may be low. Currently, there is no evidence for intrauterine transmission of SARS-CoV-2 from infected pregnant women to their fetuses, although data remain limited. WHO has recently published a scientific brief on breastfeeding and COVID-19. This brief explains that viral RNA fragments have been found by RT-PCR testing in a few breast milk samples of mothers infected with SARS-CoV-2, but studies investigating whether the virus could be isolated, have found no viable virus.
A full Q&A on the transmission of COVID-19 can be found on the WHO website. The new findings detailing the airborne transmission of the virus shows how important masks, social distancing, quarantine (among those without COVID-19), and isolation (among those currently with COVID-19) are in eradicating the virus from our daily lives.
With medical researchers around the continuing to learn about COVID-19 it is important to take scientific evidence detailing the virus seriously as more information is discovered.